
In our clinic, we often see patients who are concerned about their varicose veins, leg heaviness, swelling at the end of the day, or discomfort they cannot quite identify. Sometimes the reason is clearly visible: bulging veins in the leg, spider veins, skin changes, or a varicose vein that has gradually become larger. In other cases, the patient has symptoms but does not notice anything obvious externally.
In both situations, one point is important: looking at the leg from the outside is not always enough to understand what is happening beneath the surface.
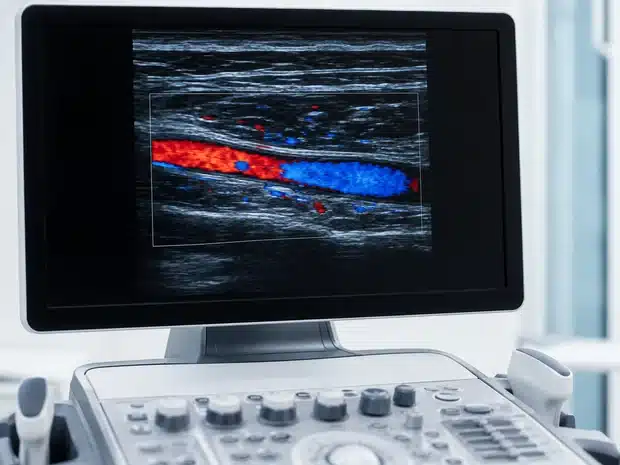
Venous Duplex ultrasound is one of the most useful tests for assessing venous circulation. It allows us to see the veins, check whether they are open, assess how blood flows through them, and detect venous reflux, thrombosis, changes from an old thrombosis, or anatomical findings that are relevant when planning treatment.
Put simply, venous Duplex ultrasound is not limited to “seeing whether there are varicose veins”. It helps answer much more important questions:
- Where do these varicose veins come from?
- Are the main veins working properly?
- Is there venous reflux?
- Is the deep venous system healthy?
- Is there any clot or evidence of previous thrombosis?
- Which treatment may make most sense in this specific case?
- Is it better to treat now, monitor the situation, or consider conservative measures?
- Is it also necessary to study veins in the pelvis or abdomen?
For this reason, at Clínica Vascular Dr. Jorge Molina, venous Duplex ultrasound is an essential part of the vascular assessment when a person comes in with varicose veins, symptoms of venous insufficiency, or suspected venous thrombosis.

Contents
- What exactly is a venous Duplex ultrasound?
- Why do the veins in the legs need a functional test?
- What does venous Duplex ultrasound assess?
- How is a venous Duplex ultrasound performed?
- Do I need to prepare in any way?
- What information does it provide before treating varicose veins?
- Venous Duplex ultrasound and thrombosis: why is it also important?
- What decisions does it help with?
- What is the “venous map”?
- Why is it not enough to “see the varicose veins”?
- Venous Duplex ultrasound in patients with recurrent varicose veins
- Duplex ultrasound and ultrasound-guided treatments
- Is it a safe test?
- When is it advisable to seek advice?
- Conclusion
- FREQUENTLY ASKED QUESTIONS
What exactly is a venous Duplex ultrasound?
A venous Duplex ultrasound is a specialised ultrasound scan used to study the veins and the flow of blood through them.
It combines two components:
- Conventional ultrasound, which allows us to see the veins and the tissues around them. It helps us assess the size of a vein, its course, whether it is dilated, whether it compresses properly, whether there are changes in its wall, or whether there is material inside the vein that could correspond to a clot.
- Doppler, which allows us to study the movement of blood. Thanks to this component, we can know which direction the blood is flowing in, whether it is flowing normally, whether there is reflux —that is, whether blood flows back down when it should not— or whether there are areas with reduced or absent flow.
In practice, venous Duplex ultrasound works as both an anatomical and functional examination. It does not only show the “shape” of the veins; it also shows “how they work”.
This distinction is fundamental in venous disease. Two people may have varicose veins that look similar at first glance but have very different venous maps. One may have reflux in the great saphenous vein; another may have varicose veins arising from superficial branches; another may have changes from a deep vein thrombosis; and another may have symptoms that are not explained by venous disease. Treatment should not be the same in all these cases.
Why do the veins in the legs need a functional test?
To understand the value of venous Duplex ultrasound, it is helpful to recall how venous circulation works.
Arteries carry blood from the heart to the tissues. Veins do the opposite: they collect blood and return it to the heart. In the legs, this task is especially demanding because blood has to rise from the feet upwards, against gravity.
To achieve this, the body uses several mechanisms. One of the most important is the contraction of the calf muscles while walking, which helps “push” blood upwards. Another key mechanism is the venous valves, small structures inside the veins that allow blood to move up but make it difficult for it to flow back down.
When these valves fail, blood may flow in the opposite direction for part of the time. We call this venous reflux. This reflux increases pressure inside the superficial veins, promotes their dilation, and may lead to varicose veins, heaviness, swelling, cramps, itching, skin changes, or, in more advanced cases, venous ulcers.
The problem is that venous reflux is not always visible externally. We may see a varicose vein but not know where it originates. We may see a swollen leg but not know whether the cause is venous, lymphatic, general medical, orthopaedic, or another type of problem. We may suspect venous insufficiency, but we need to check which veins are involved.
This is where venous Duplex ultrasound provides decisive information.

What does venous Duplex ultrasound assess?
Venous Duplex ultrasound makes it possible to assess several important aspects.
1. Venous anatomy
Each person has their own “venous map”. There are main veins, branches, connections between systems, and anatomical variants. Duplex ultrasound helps identify which veins are present, where they run, and how they relate to the visible varicose veins.
When studying varicose veins in the legs, particular attention is paid to the superficial venous system, which includes the saphenous veins and their branches, and to the deep venous system, which carries most of the venous return from the limb.
Perforating veins, which connect the superficial system with the deep system, can also be assessed. In some patients these veins may be clinically relevant, especially if there is reflux or advanced venous disease.
2. Whether the veins are open or blocked
A healthy vein should be patent, meaning open to blood flow. During the examination, the specialist can gently compress the vein with the transducer to check whether it collapses normally. This manoeuvre is very useful for assessing the presence of clots in certain venous segments.
When a vein does not compress well or material appears inside it, there may be a thrombosis or a residual change from a previous thrombosis. This information completely changes the diagnostic and treatment approach.
3. The direction of blood flow
Doppler allows us to see whether blood is flowing in the right direction. In the veins of the legs, under normal conditions, flow should be directed towards the heart. If certain manoeuvres cause reverse flow to appear for a significant period of time, we call this venous reflux.
Reflux may affect superficial, deep, or perforating veins. It may also be limited to a specific segment or extend along a venous trunk, such as the saphenous veins.
4. Flow speed and pattern
It is not only important whether there is flow or not. How that flow behaves also matters. Duplex ultrasound can show patterns that suggest obstruction, difficulty with drainage, or haemodynamic changes.
For example, in some cases with symptoms or signs suggesting venous obstruction above the groin, it may be necessary to extend the study to the abdominal or pelvic veins, or to consider other imaging tests. This is not decided as a routine measure, but according to the medical history, physical examination, and the findings of the Duplex ultrasound itself.
5. Vein diameter
The size of a vein also provides information. A dilated vein may be associated with valve incompetence or a greater burden of venous disease. Diameter helps when planning treatments, choosing the most appropriate technique, and assessing technical details if an endovenous procedure is being considered.
6. The relationship between symptoms and findings
This point is very important. Finding reflux on an ultrasound does not automatically mean that a vein must be treated. The result must be interpreted together with the patient’s symptoms, examination, and clinical context.
In vascular medicine, we do not treat isolated images: we treat people. Duplex ultrasound helps us understand whether what we see explains what the patient feels and whether acting on that vein makes clinical sense.
How is a venous Duplex ultrasound performed?
Venous Duplex ultrasound is a non-invasive, painless test that does not use radiation. It does not require injections, contrast, or anaesthesia.
The patient is positioned so that the specialist can access the areas that need to be examined. When assessing venous insufficiency and varicose veins, it is often performed with the patient standing, whenever possible. There is a very logical reason for this: venous insufficiency tends to show itself especially when blood has to rise against gravity, that is, when we are standing or sitting. Studying the veins in a position that better reproduces this situation allows reflux to be assessed more appropriately.
At certain points, the patient may be lying down, for example if suspected deep vein thrombosis is being assessed or if specific segments need to be examined. The exact position depends on the reason for the test.
During the examination, the specialist applies gel to the skin and moves the transducer over different areas of the leg: groin, thigh, knee, calf, ankle, or areas where varicose veins are seen. The ultrasound machine shows real-time images.
It is common to perform manoeuvres to provoke or assess flow, such as asking the patient to perform a Valsalva manoeuvre —similar to straining with the abdomen— or gently compressing areas of the leg to observe the venous flow response. These manoeuvres help detect reflux and locate its origin.
The duration may vary depending on the case. A simple study of spider veins with few symptoms is not the same as a complex assessment of recurrent varicose veins, suspected previous thrombosis, skin changes, or possible pelvic involvement. What matters is not doing the test quickly, but doing it well and obtaining useful information for decision-making.

Do I need to prepare in any way?
In most cases, no special preparation is needed.
It is usually not necessary to fast. It is advisable to wear comfortable clothing that is easy to remove or pull up, so the legs can be examined. If the patient wears compression stockings, they should follow the instructions given by the clinic according to the reason for the study.
It is also useful to bring relevant medical information: previous reports, results of earlier ultrasound scans, a history of thrombosis, varicose vein treatments already performed, previous surgery, anticoagulant medication if applicable, or any information that may help interpret the examination more accurately.
In clinic, we often see that a small detail in the medical history changes how the Duplex ultrasound is interpreted. For example, a primary varicose vein is not the same as a varicose vein that appears after a deep vein thrombosis. Studying varicose veins for the first time is also different from studying a recurrence after previous treatment.
What information does it provide before treating varicose veins?
Venous Duplex ultrasound is especially important before treating varicose veins because it allows a personalised strategy to be designed.
We can see bulging veins at first glance, but we do not always know which vein is feeding them. If only the visible varicose vein is treated without identifying the origin of the reflux, the treatment may be incomplete or less durable.
Duplex ultrasound helps answer questions such as:
- Is there reflux in the great saphenous vein?
- Is the small saphenous vein involved?
- Are there varicose branches arising from a saphenous vein or from another source?
- Are there relevant perforating veins?
- Is the deep venous system patent?
- Is there evidence of old thrombosis?
- Does the anatomy allow endovenous treatment?
- Does the vein diameter point towards one technique or another?
- Is it better to treat a venous trunk, varicose branches, spider veins, or combine approaches?
- Is it advisable to monitor before intervening?
This information may influence the indication for treatments such as radiofrequency, VenaSeal®, sclerotherapy, phlebectomy, or other options. It is not about choosing a technique because it is fashionable, but about choosing the most reasonable option according to the venous map and the patient’s clinical situation.
At Clínica Vascular Dr. Jorge Molina, venous Duplex ultrasound makes it possible to explain to the patient what has been found and why a specific strategy is being proposed. This explanation is key to shared, realistic decision-making.

Venous Duplex ultrasound and thrombosis: why is it also important?
Duplex ultrasound is not only used to study varicose veins. It is also a fundamental tool when venous thrombosis is suspected.
Deep vein thrombosis occurs when a clot forms inside a deep vein. It may cause swelling, pain, increased temperature, colour changes, or a feeling of tightness in the leg, although symptoms vary greatly from one person to another. If it is suspected, assessment must be carried out by a doctor.
Duplex ultrasound allows us to look inside the vein, assess whether it compresses, check whether there is flow, and detect signs compatible with a clot. It can also help assess changes from an old thrombosis, such as partially recanalised veins, changes in the wall, or alterations in flow.
This information is important because thrombosis changes treatment and follow-up. In addition, previous thrombosis may damage venous valves and favour later problems with venous return, swelling, or secondary varicose veins.
In the event of sudden symptoms, significant pain, marked swelling, shortness of breath, chest pain, or suspected pulmonary embolism, you should not wait for a scheduled appointment: you should seek urgent medical attention.
What decisions does it help with?
Venous Duplex ultrasound is not an isolated test that is “put away in a drawer”. Its real value lies in how it helps guide decisions.
Confirming or ruling out venous disease
Sometimes symptoms fit very well with venous insufficiency: heaviness at the end of the day, worsening with heat, relief when elevating the legs, evening swelling, visible varicose veins. In other cases, however, it is not so clear.
Duplex ultrasound helps confirm whether there is reflux, obstruction, or thrombosis, or whether the findings do not justify the symptoms. When there is no clear venous cause, it may point towards the need to consider other possibilities.
Classifying severity
Not all venous diseases are at the same stage. There may be spider veins, reticular veins, varicose veins, swelling, skin changes, or venous ulcers. Duplex ultrasound, together with the clinical examination, helps assess the extent of the problem.
This is not done merely to attach labels, but to estimate risks, prioritise decisions, and explain to the patient what is happening.
Planning treatment
If treatment is decided, Duplex ultrasound helps plan the procedure. It shows which vein should be treated, where the diseased segment begins and ends, its diameter, its course, its relationship with other structures, and which varicose branches depend on it.
In endovenous treatments, such as radiofrequency or VenaSeal®, this planning is essential. It is also important in sclerotherapy, especially if there are larger varicose veins or if ultrasound guidance is needed.
Avoiding unnecessary treatments
A good test also helps us say “this should not be treated in this way”, “there is no need to intervene at this time”, or “the symptoms the patient describes are NOT being caused by venous disease, but have another origin (bones, muscles, spinal problems…)”.
For example, when performing Duplex ultrasound before treatment in a patient with spider veins, we may find:
- Findings suggesting that, if we treat them, the treatment will probably fail (in which case we can be honest and advise the patient against it).
- Findings that directly contraindicate treatment (that is, if we were to perform the treatment, we would run a significant risk of causing some type of harm to the patient).
- Venous insufficiency that is not visible at first glance and makes it advisable to treat first (varicose vein treatment), so that treatment of the spider veins can later be successful.
- Findings that recommend caution or further studies.
Personalising expectations
Duplex ultrasound allows us to explain more clearly what can be expected from treatment. Treating isolated spider veins is not the same as treating varicose veins that depend on an insufficient saphenous trunk. Nor is a first procedure the same as recurrent varicose veins after previous treatments.
Clear information avoids unrealistic promises and helps decisions be made calmly.
Deciding on follow-up
In some patients, especially if symptoms are mild, if there are contraindications, if the patient prefers a conservative approach, or if the findings do not justify an intervention, follow-up and conservative measures may be considered.
Duplex ultrasound serves as a starting point for future comparison if there is progression, new reflux, or relevant changes.
What is the “venous map”?
When we talk about a “venous map”, we mean a representation of how the veins in a leg are organised and where the points of reflux or abnormality are located.
This map is not always given to the patient as a formal drawing, but it does guide the medical decision. It identifies the main veins, their branches, insufficient segments, relevant connections, visible varicose areas, and areas that may require treatment. It is best imagined as a “mental map of the 3D venous labyrinth” that the vascular surgeon builds in their head to guide decisions and treatments.
In varicose veins, the venous map is comparable to the plan of an installation before repairing it. If we only see the external “leak”, we can act on what is visible. But if we do not know where the pressure feeding that leak comes from, treatment may fall short.
Why is it not enough to “see the varicose veins”?
Varicose veins are dilated superficial veins. They are often diagnosed visually because they can be seen and felt. But diagnosing that “there are varicose veins” is not the same as understanding that person’s venous disease.
There are several reasons:
- Venous insufficiency may exist without large visible varicose veins.
- Varicose veins may be primary or secondary.
- The deep venous system may be normal or may have residual changes.
- The vein causing the reflux may not match the most visible varicose vein.
- Recurrent varicose veins may appear after previous treatments.
- There may be leg symptoms that are not venous in origin.
- Pelvic or abdominal disease may be present in specific cases.
- There may be superficial or deep thrombosis requiring a different approach.
For this reason, before deciding on treatment for varicose veins, the prudent approach is to study venous anatomy and function correctly.
Venous Duplex ultrasound in patients with recurrent varicose veins
Varicose veins may reappear or develop in new areas over time. This may happen for different reasons: natural progression of the disease, recanalisation of a treated vein, appearance of new points of reflux, development of varicose branches, or problems not detected in an initial study.
In these cases, Duplex ultrasound is especially useful. It makes it possible to distinguish whether the current varicose vein depends on a vein that has already been treated, a different vein, a perforating vein, a pelvic origin, or a deep abnormality. This distinction is important because treatment of recurrent varicose veins should not be based only on what was done years ago, but on what is found now.
Duplex ultrasound and ultrasound-guided treatments
Duplex ultrasound is not only used for diagnosis. In many venous treatments, it is also used as a guide.
It allows a vein to be located precisely, the position of a needle or catheter to be controlled, the course of a saphenous vein to be followed, safety distances to be checked, and specific steps of the procedure to be verified. This is common in endovenous techniques and in ultrasound-guided sclerotherapy.
Ultrasound has changed the way venous disease is treated because it allows procedures to be more targeted, more anatomical, and more personalised. Even so, each technique has its indications, limitations, and possible side effects, which must be explained during the consultation.
Is it a safe test?
Yes. Venous Duplex ultrasound is a non-invasive test and does not use ionising radiation. It does not require contrast and does not cause pain. It may be somewhat uncomfortable if a sensitive area needs to be compressed, but this usually only happens in patients with pain, inflammation, or suspected thrombosis or phlebitis.
As with any medical examination, its usefulness depends on it being properly indicated, properly performed, and properly interpreted. Technology is important, but the professional’s experience is important too.
When is it advisable to seek advice?
It is advisable to request a vascular assessment if you have visible varicose veins, frequent heaviness, leg swelling, cramps, itching, a sensation of heat, skin colour changes, a history of thrombosis, progressive varicose veins, discomfort that worsens when standing, or questions about previous treatments.
It is also advisable to seek advice if complications appear, such as bleeding from a varicose vein, painful hardening of a superficial vein, skin changes around the ankle, or wounds that take a long time to heal.
And, of course, if sudden swelling of one leg, significant pain, or suspected thrombosis appears, the assessment should be urgent.
Conclusion
Venous Duplex ultrasound is a key test for understanding venous circulation in the legs. It allows the veins to be seen, flow to be studied, reflux to be detected, thrombosis or old residual changes to be assessed, superficial and deep problems to be differentiated, and treatments to be planned in a personalised way.
In varicose veins, its value lies not only in confirming what can already be seen externally, but in discovering the origin of the problem. In thrombosis, it helps establish a diagnosis and guide medical decisions. In follow-up, it allows changes, recurrences, or evolution after treatment to be assessed.
In clinic, a good venous Duplex ultrasound examination makes it possible to explain the problem more clearly, avoid unnecessary treatments, and choose a prudent strategy for each case.
If you have varicose veins, symptoms of venous insufficiency, or questions about your circulation, request an assessment with a specialist in Angiology and Vascular Surgery.
Notice: this information is general and does not replace a personalised medical consultation. Diagnosis and treatment must be individualised after assessment by a qualified healthcare professional.
FREQUENTLY ASKED QUESTIONS
Does venous Duplex ultrasound hurt?
It usually does not hurt. It is an ultrasound scan performed on the skin with gel and a transducer. There may be pressure in some areas, but it is a test that is generally very well tolerated.
Does it involve radiation?
NO. Duplex ultrasound uses ultrasound waves, not radiation.
Do I need to fast?
For a venous Duplex ultrasound of the legs, fasting is usually not necessary.
Why is it sometimes performed standing?
Because venous reflux is more clearly demonstrated when blood has to rise against gravity. When studying venous insufficiency and varicose veins, the standing position usually provides more reliable information.
Can it diagnose thrombosis?
YES, it is a fundamental test in the diagnosis of venous thrombosis in the legs, always within an appropriate medical assessment.
Does it help decide varicose vein treatment?
YES. In most cases, it provides essential information to diagnose the problem, locate the origin of the reflux, and plan treatment.
Is Duplex ultrasound always needed when there are spider veins?
YES. Before deciding on treatment for spider veins, it is necessary to rule out certain problems that could make that treatment ineffective or even dangerous for the patient, or that could make it more advisable to plan the order of treatments differently.
Can it be normal even if I have symptoms?
YES. Not all leg discomfort is due to venous disease. If Duplex ultrasound does not show abnormalities that explain the symptoms, other causes may need to be assessed.
Does the result mean I have to have surgery?
NO. Duplex ultrasound helps guide decisions, but the indication for treatment depends on the symptoms, signs, clinical context, patient preferences, and the specialist’s assessment.
Should you be interested in getting to know this disease better, and its causes, consequences, how to treat them, and, even better, what can we do to prevent them, you can find it all well explained in the ebook VARICOSE VEINS: Truth & myths.