During the last years – always pursuing the target of a less aggressive, less invasive approach in the treatment of varicose veins -, new techniques have been developed, based on the same principles I was explaining in the previous post: the use of puncture-catheter to navigate inside the varicose vein, visual guide by Duplex Ultrasound, controlled lesion of the varicose vein from inside (endovenous), minimal use of anesthesia (local), outpatient procedure, etc. But over all these advantages we have tried to add one more, which is the possibility to perform it almost without anesthesia, and eventually even without the need of an operating theater (in a medicalized office).
The key point in this evolution is based on the search for a method that would allow us a similar controlled injury of the varicose vein, but without the need of heating it; this way, if there is no heat release, we won’t have the need to fill the surroundings of the varicose vein with anesthetic fluid to act as a “heat sink”, and therefore, we will save the patient several anesthetic punctures.
The techniques that are available and with valid mid-term scientific results, as of 2018, are mainly two: the use of glue, and the mechanical-chemical ablation (MOCA).
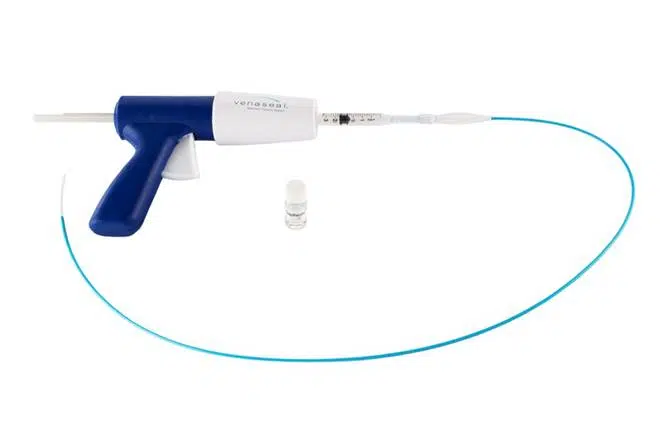
Glue (VenaSeal®)
There are several different brands that manufacture treatments with glue, but I’m mentioning explicitly VenaSeal® (from Medtronic®) because, as of today, it’s the one with more and better quality scientific studies that avail its efficacy and safety, and thus, it’s the most broadly used.
The first part of the treatment is common to those that I explained in the previous post: we insert a catheter (a long, thin plastic tube) inside the varicose vein through a puncture (or a small incision), either at the ankle or near the knee (with the visual guide of the Duplex Ultrasound). Then we navigate ascending the catheter inside the vein until shortly before the great saphenous vein joins the common femoral vein (the safenofemoral junction, in the groin).
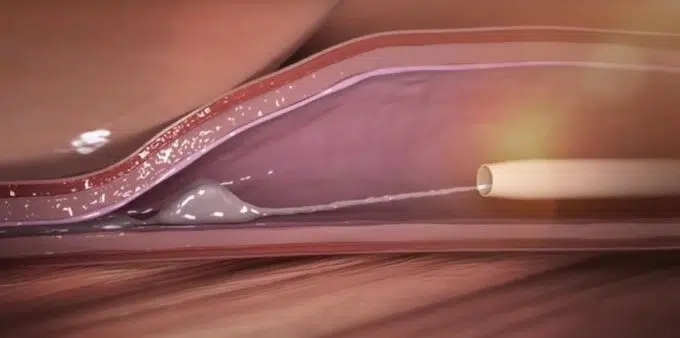
Then, using a very precise control mechanism, we start deploying a highly adhesive glue inside the vein (actually, the glue that we use is cyanoacrylate, the same component the famous Loctite® has, but according to the explanations of the manufacturer, it has been reformulated in a way that it is perfectly biocompatible: after all, we are releasing it inside a vein…). This cyanoacrylate will cause not only the varicose vein walls to stick together, but also will damage them to trigger the healing mechanism that will transform the varicose vein into a scar, which eventually will be reabsorbed by the body over time.
The amount of cyanoacrylate being used in this procedure is really low, and according to the manufacturer, it will be reabsorbed by the body in approximately one year.
The post-procedural stage is generally very light, with no need of compression stockings, and immediate regain of usual activities. However, it should be pointed out that a small amount of patients may present with pain along the treated area during the first few days because of the inflammation generated by the glue. If this happens, this can usually be controlled without major problems with usual painkillers.
The scientific studies that are available so far are mid-term (follow up of about 2 years), and are quite optimistic regarding this technique, showing results that are comparable to those of laser and radiofrequency.
Following this, the official video from Medtronic® (as we said, the manufacturer of VenaSeal®), that will help illustrating the procedure:
Mechanical-Chemical Ablation or MOCA (ClariVein®)
In this case, I’m explicitly mentioning the trade mark of the device because it’s the best known and, as of today, it’s the only manufacturer that provides it.
The first part of the treatment is also common to the previous ones: we insert a catheter inside the varicose vein through a puncture (or a small incision), either at the ankle or near the knee (with the visual guide of the Duplex Ultrasound). Then we navigate ascending the catheter inside the vein until shortly before the great saphenous vein joins the common femoral vein (the safenofemoral junction, in the groin).
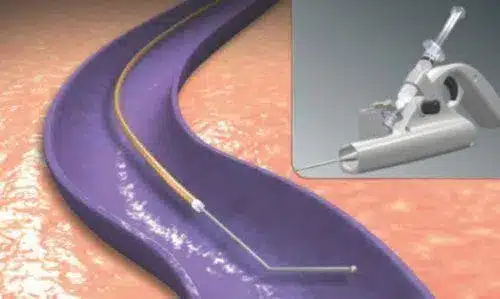
Once located at the appropriate spot, the catheter uses a very ingenious mechanism: the tip starts rotating at a very high speed, “peeling” the inner layer of the vein (the endothelium) in a virtually painless way, and simultaneously spraying the same drug that we use for sclerotherapy (polidocanol), only that being released by a tip which is rotating so fast, centrifugal force pushes it inside the wall of the vein, greatly increasing its effectiveness. Then the vein contracts and occludes, similarly to the previous treatments.
Despite using local anesthesia just at the entry site, the patient only feels a slight vibration along the treated area (similar to the feeling of having a mobile phone vibrating inside the trouser’s pocket); eventually, a little pull can be felt but, generally speaking, it’s also a painless technique.
Similar to the previous one, the scientific studies that are available so far are mid-term (follow up of about 2 years), and are quite optimistic regarding this technique, showing results that are comparable to those of laser, radiofrequency and VenaSeal®.
Following this, the official video from the distributor of ClariVein®, that will help illustrating the procedure:
Should you be interested in getting to know this disease better, and its causes, consequences, how to treat them, and, even better, what can we do to prevent them, you can find it all well explained in the ebook VARICOSE VEINS: Truth & myths.