
Sclerotherapy is one of the treatments that raises the most questions when we talk about spider veins. It may look like a simple procedure, but it is important to understand what it can achieve, what it cannot promise, and which precautions matter before deciding to go ahead.
In this article we will focus on sclerotherapy for spider veins. Sclerotherapy can also be used for other venous problems, such as certain varicose veins, vascular malformations, or venous ulcers, but that is not the purpose of this explanation. Here we will discuss the small visible veins in the skin, how they are treated, and the care needed to reduce risks.
Contents
- What are spider veins?
- Why do they appear?
- How are they related to varicose veins?
- What consequences do spider veins have?
- What does sclerotherapy involve?
- What are the sessions like, and when are results visible?
- Possible side effects
- Post-sclerotherapy pigmentation
- Can pigmentation be prevented?
- And, having said that, what happens if pigmentation appears?
- Can pigmentation be removed?
- Precautions before treating spider veins
- FREQUENTLY ASKED QUESTIONS
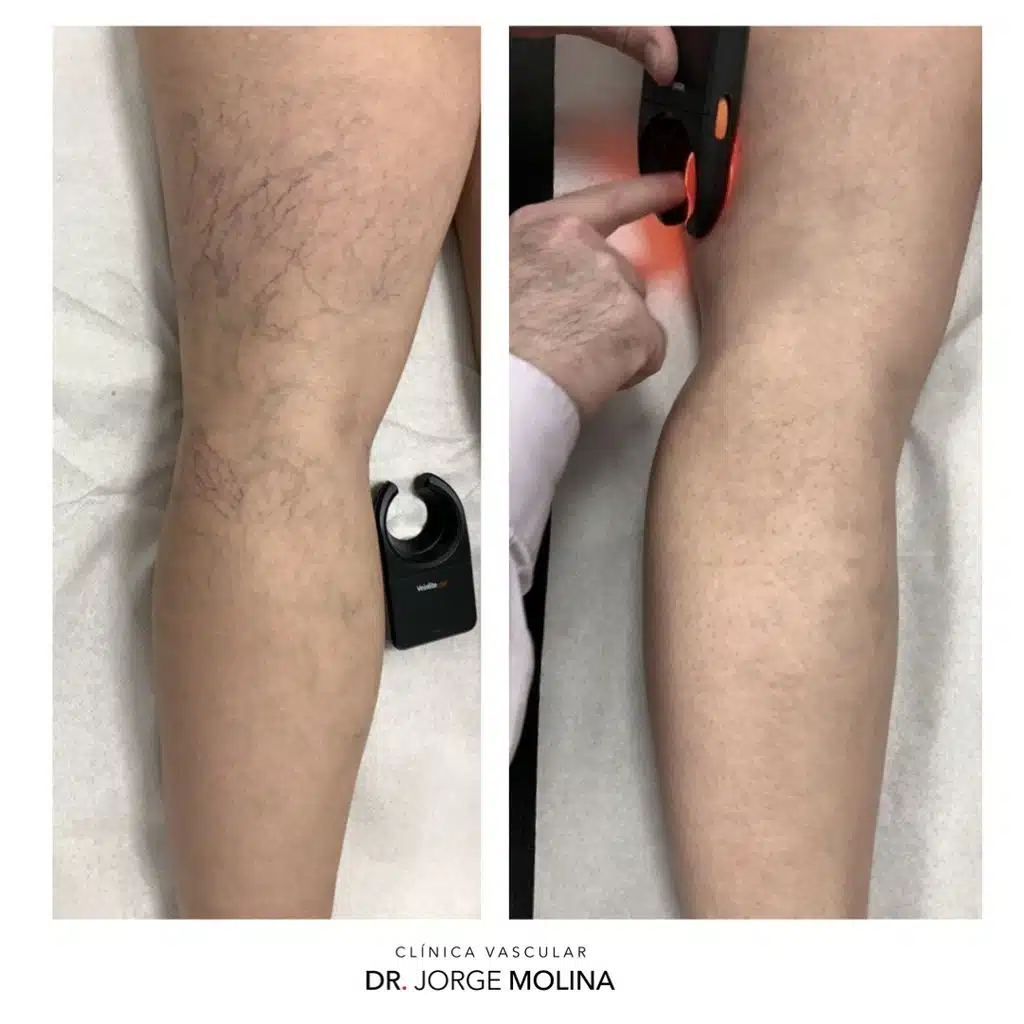
What are spider veins?
Put very simply, spider veins are skin capillaries that have dilated enough to become visible.
We can imagine the skin as a huge radiator made up of millions of microscopic capillaries, interconnected in a large network. When some of those capillaries dilate enough, they stop being invisible and appear as fine reddish, bluish, or greenish lines.
They are a very common reason for consultation, and many misconceptions circulate around them. We are always talking about vessels less than 2 millimetres in diameter, located within the skin, not underneath it. This matters because it distinguishes them from varicose veins, which come from the superficial venous system and are located deeper down.
From a practical point of view, we usually distinguish two types: reticular veins, which are slightly thicker and bluish or greenish in colour, and telangiectasias, which are much finer, sometimes as thin as a hair, and wine-red in colour. They sometimes appear together, forming patterns that look like branches or small spider webs.
Why do they appear?
The truth is that we do not know precisely all the mechanisms that explain why they appear. A great deal has been written about spider veins, but much of what is said has no clear scientific basis. Even so, several factors seem reasonably likely to play a role.
- Genetic factor: some people seem to have greater capillary fragility. This does not necessarily mean it is hereditary, but rather that they were born with capillary walls that are more prone to dilating. This factor is often associated with other characteristics, such as having thin skin (although not always) or developing small bruises after minor knocks, or even spontaneously
- Hormonal factor: female hormones may favour the dilation of these capillaries in predisposed people. This helps explain why they are more common in women, during pregnancy, or with certain hormonal treatments such as contraceptive pills. Other hormones such as steroids (especially corticoids or corticosteroids) may also be involved.
- Excess weight: increased fat in the lower limbs can make the tissues looser and less resistant, favouring capillary dilation.
- Age: over the years, the skin and small vessels become more fragile, as happens with many tissues in the body.
Although they are often considered directly related to varicose veins, in general this is not the case: some people have varicose veins without spider veins, and others have spider veins without varicose veins.
How are they related to varicose veins?
In general, spider veins are not small varicose veins. They are different vessels and are located in a different place. Varicose veins are veins of the superficial venous system, located under the skin. Spider veins are dilated capillaries within the skin itself.

The important practical relationship is different: if a person has both varicose veins or venous insufficiency and spider veins in the same limb, the correct order of treatment must always go from the largest vessel to the smallest. First the varicose veins are assessed and, if appropriate, treated; then the reticular veins; and finally the telangiectasias.
That is why it is so important to perform a venous Duplex Ultrasound before starting an aesthetic treatment for spider veins. If we try to close capillaries over a venous network with increased pressure:
- The chance of success will be lower.
- The chance of recurrence (that is, that they come back) will be higher.
- The risk of adverse effects may also increase (phlebitis of a varicose vein, thrombosis, skin pigmentation, etc).
What consequences do spider veins have?
Here it is worth being very clear, because there is a lot of doubtful, incorrect, or deliberately confusing information. Spider veins, by themselves, are usually not a health problem.
- Spider veins NEVER cause any symptoms: they do not cause pain, heaviness, or swelling. They are too small to cause those symptoms. If there is discomfort in the leg, another cause must be looked for: true venous insufficiency, muscle problems, sciatica, joint problems, or other conditions.
- Spider veins will NEVER grow into varicose veins. They are different vessels and are found in another layer of the body.
- Spider veins are not dangerous and do not cause important complications. The rare exception would be some thicker reticular veins, connected to a varicose vein and very superficial, which could bleed if they receive a blow or intense rubbing.
So what is the main problem? Aesthetic appearance. They can be visible, bothersome for the person who has them, and affect how the legs are perceived, but they should not be presented as a disease, much less a serious one.
What does sclerotherapy involve?
We have distinguished two types of spider veins: reticular veins (thicker, although always under 2 mm, and greenish-blue in colour) and telangiectasias (very fine and wine-red in colour). Reticular veins can be removed effectively and safely with sclerotherapy. Telangiectasias, which are much finer (sometimes even smaller than the needle used for sclerotherapy injection, and therefore cannot be injected), can be treated with laser (this is a treatment that should be performed at the very end, once all sclerotherapy treatment has been completed, and we will not cover it in this article for reasons of length).
Sclerotherapy consists of injecting an irritating medication into the reticular vein to make it close. External compression is then applied, usually with a compression stocking, to help the small vein close while empty and reduce the likelihood of side effects.
The injection should be virtually painless, like a mild mosquito bite. If it is very uncomfortable, you should tell the doctor immediately, because it may indicate that the injection is not being given exactly where it should be.
The most commonly used medications are polidocanol, sodium tetradecyl sulfate, or chromated glycerin, with polidocanol being the most widely used in Spain. In our practice we use polidocanol because it offers a good balance between efficacy, tolerability during injection, and side-effect profile.
The medication causes controlled damage to the inner layer of the small vein, called the endothelium. Over the following days or weeks, and with the help of compression, the body ends up sticking its walls together through a small fibrosis. In practice, this tiny scar makes the small vein stop being visible.
What are the sessions like, and when are results visible?
Sclerotherapy is performed in sessions. Because a medication is administered, we cannot inject as much as we want. All medications have a maximum dose and, when they are injected into a vein, that limit must be respected with particular care.
When we use polidocanol, a generally accepted safe amount is one 2 ml ampoule every 24 hours at most.


We use it in the form of microfoam: the liquid medication is mixed with air to obtain a fine foam, similar to meringue, which allows a larger area to be treated with a smaller amount of medication.
- Microfoam has greater ability to close veins than the unfoamed liquid.
- The 2 ml of medication can become approximately 7-8 ml of microfoam, allowing more reticular veins to be treated in each session.
- There is also a limit to the amount of air that can be injected, so the technique must be performed with judgement and experience.
If all the small veins cannot be treated in a single session, when can I continue with the next one? Well, we have said that the dose limit applies every 24 hours, correct? After 24 hours we could continue treatment with another session using the same maximum dose (in an area that has not yet been treated).
One VERY IMPORTANT point to keep in mind is that results are not immediate. They start to be assessable after 4 to 6 weeks. That is why we usually review at 6-8 weeks, when it can already be decided whether the result is sufficient or whether a touch-up session may be advisable.


In practical terms, and to avoid keeping the patient tied up with this treatment for a long time, when someone needs more than one session, our advice is to carry out all the sessions needed to complete both legs as close together as possible. This way, both complete legs go through those 6-8 weeks until the review, and at that appointment both legs can be reviewed in full at the same time.
And how many sessions will be needed? We cannot know in advance. It will depend on many factors: the number of small veins to be treated, how they respond to treatment (the response can vary considerably from one person to another, or even from one day to another in the same patient), and how the patient sees the result. That is why we do not sell “packs” of sessions or anything similar, because we treat patients: we prefer each person to be able to assess how things are going, and to always have the freedom to decide whether to stop or continue.


During those weeks, the treated small veins may change colour, become reddish or purple, small bruises may appear, or they may even become temporarily more visible and firm to the touch. In many cases this is a small clot inside the treated vein. It is not usually dangerous, but it may take longer to be reabsorbed (3-4 MONTHS) and slightly increases the possibility of pigmentation.
Whether the treated reticular veins close while empty (the ideal situation) or by trapping a small clot will depend largely on how strict the patient is with the compression stocking, and on avoiding exertion or sport (except walking, which is mandatory) during the first few days. It is also true, however, that this can sometimes happen even when everything is done correctly. If this phenomenon occurs, there is only one solution: patience, a great deal of patience, until it finally resolves (the body ends up dissolving the small clot and takes the little vein with it).

At the end of each session, even before you get up from the examination couch, we will put on a compression stocking, which you will need to use for about 3 weeks (we will give you a prescription so you can bring the exact brand and model you will need; we do not want mistakes). The reason is that several studies have shown that using a compression stocking improves treatment efficacy, but above all reduces the likelihood and severity of possible side effects, which is why we consider it essential (in other words, we do not perform the treatment without the stocking).
Possible side effects
Sclerotherapy, when it is properly indicated and performed by an experienced professional, is a safe, low-risk procedure. But no medical treatment is free from possible side effects.
- Allergy to the medication: as with any drug, this can occur. Allergy to polidocanol is uncommon (much less common than allergy to Penicillin or Nolotil, to give a couple of examples) and, when it appears, it is usually mild, with hives or itching that resolve within hours or days. Severe reactions are very rare.
- Skin pigmentation: this is the most important cosmetic side effect and the most characteristic one of this treatment.
- Matting: the appearance of very small telangiectasias around a treated reticular vein. It usually improves on its own, at least partially, over the following months.
- Skin necrosis, or even necrosis of the subcutaneous tissues: this is extremely rare if the technique is performed correctly, but the risk increases greatly if the technique is carried out by non-expert personnel.
- Phlebitis: (formation of a thrombus in a superficial vein): it is uncommon if the technique is well performed, if the patient uses the elastic stocking correctly, and if they go out walking and remain active. It is not very dangerous, although it can be very painful. If it is suspected, the doctor should be consulted immediately and treatment started to resolve it.
- Deep vein thrombosis (formation of a thrombus in a deep vein): this is a potentially much more serious situation than the previous one, and it is even rarer for it to occur PROVIDED THE TECHNIQUE HAS BEEN PERFORMED PROPERLY (among other reasons, this is why a prior Duplex Ultrasound study is needed, and why the technique must be carried out by an experienced professional). Using elastic stockings as prescribed, walking, and leading an active life are factors that protect very effectively against this possibility.
Most complications are related to poor injection technique (which is why the experience of the doctor performing the treatment is so important, including knowing the “forbidden” areas where injection should not be performed, the prior study, and so on), an inappropriate indication, or not following the post-treatment measures. Pigmentation, however, can appear even when everything is done correctly, both by the doctor and by the patient.
Post-sclerotherapy pigmentation
Post-sclerotherapy pigmentation is a brown or ochre stain that follows the course of one or more treated veins. It may be subtle, but in some cases it remains visible even after the small vein has already been reabsorbed.

Pigmentation seems to be influenced by certain genetic factors, and therefore it is only predictable when a person has already experienced it before, or when it is known that, after a bruise, they do not reabsorb it completely and some mark remains (the phenomenon is similar, due to incomplete chemical degradation of the haemoglobin in the red blood cells of the bruise, and therefore pigmentation is more likely to occur with sclerotherapy treatment as well). It may also be more likely if the patient has previously had scars (from accidental or surgical wounds) that remained pigmented. In all these cases, the doctor should be told before treatment so they can advise whether it is appropriate to proceed.
One factor that greatly influences the possibility of pigmentation is sun exposure, which is why we advise against performing this treatment in summer. In fact, it is not entirely clear whether direct sun exposure alone is responsible, because two other factors may also be involved:
1.- Sun rays can pass through clothing, especially the thinner and cooler fabrics we usually wear in summer (linen, cotton, etc), so this does not really protect against the action of the sun or, therefore, against pigmentation.
2.- There may also be another related factor, such as melanin synthesis and its regulation by other hormones (MSH, or melanocyte-stimulating hormone, and melatonin), which the body produces according to its perception of daylight hours. In summer, because the eye perceives more hours of light, a part of our brain called the hypothalamic-pituitary axis adjusts its synthesis of MSH hormone (and other regulatory mechanisms, which also intervene in the sleep-wake cycle, reproductive cycle, etc). It is possible (although not yet definitively proven) that this increases the skin’s predisposition to produce melanin (the pigment that tans us), and that this may also be a factor that increases the chances of developing pigmentation after sclerotherapy, even if the sun has not shone directly on the treated legs.
In practical terms, we advise against leaving the legs uncovered (even simply walking down the street wearing shorts) during the TWO MONTHS after sclerotherapy treatment. This means that, for patients who will be in our latitude, we stop performing these treatments in mid-April (any sun exposure would have to be avoided until mid-June; we have said two months) and resume them towards the end of September.
Of course, if you plan to travel to tropical destinations during our autumn or winter, where you will wear short clothing and may be exposed to the sun, keep this in mind because we should not perform this treatment in the two months before the trip.
Can pigmentation be prevented?
Unfortunately, in many cases it cannot be prevented. In other words, even when everything is done properly (both by the doctor and by the patient following every instruction exactly), it can still happen. But there are two essential things you can do to greatly reduce the likelihood of pigmentation appearing:
1.- Avoid sun exposure, or avoid having the treatment in summer or just before summer (as explained above).
2.- Use the elastic stockings correctly and strictly, exactly as your doctor advised. In our case, we put the stocking on immediately after the session and recommend keeping it on without removing it at all for the first 24 hours or slightly longer (until bedtime the following day). From then on, put them on before getting out of bed, wear them throughout the day, and remove them only when going back to sleep (for 3 weeks), except for the minimum time needed to shower.
When used properly, compression stockings protect quite effectively against most of the side effects described above, and they considerably reduce (although not completely) the likelihood of developing pigmentation.
From everything explained above, there is something very important that I want you to understand clearly: NO SPECIFIC COSMETIC RESULT CAN BE GUARANTEED, as with everything in Medicine, because some factors are beyond our control, and IT CANNOT BE GUARANTEED THAT POST-SCLEROTHERAPY PIGMENTATION WILL NOT APPEAR. If you want us to perform this treatment, we will do everything possible to minimise this likelihood, but you must accept the possibility that it may still occur, at your own risk.
And, having said that, what happens if pigmentation appears?
Well, after how alarming this may have sounded, the reality is that most pigmentation will eventually disappear on its own. But it takes time.
It is estimated that in around 80% of people who develop pigmentation, it eventually disappears spontaneously (completely or partially) after 1 year. This means that up to 20% of people with pigmentation do not fully reabsorb it after one year and it may remain “permanent”.

If pigmentation appears, sun exposure should be avoided using SPF 50+ sunscreen creams, because pigmented areas tend to darken even more, and this may help fix the pigmentation.
Can pigmentation be removed?
The good news is that YES. There are some Intense Pulsed Light treatments (IPL – VPL) which, in expert hands, have achieved very good results in removing post-sclerotherapy pigmentation. We use them as a last resort in cases where, after a reasonable period of time, we see that the pigmentation is not disappearing on its own.
Precautions before treating spider veins
Although, in general, sclerotherapy is a simple, low-risk treatment, there are certain situations in which special precautions are needed (or in which the treatment should simply not be performed):
- Pregnancy: it has not been proven that injecting these medications cannot have a harmful effect on the foetus, so they should be avoided. In addition, during pregnancy it is most likely that more varicose veins and spider veins will appear, and that after delivery at least some of them will disappear spontaneously, so performing this treatment would be pointless. Finally, bearing in mind that the purpose is exclusively aesthetic and not to treat a disease, it can be delayed and scheduled calmly outside pregnancy. Therefore, if you think you might be pregnant, please tell your doctor immediately so this treatment can be cancelled.
- Breastfeeding: similarly, it has not been proven that these medications cannot pass to the baby through breast milk and cause harm. Again, as this is a purely aesthetic treatment, it can be postponed without any problem, so if you are breastfeeding, please tell your doctor immediately so this treatment can be cancelled.
- Flights: as with all treatments related to varicose veins, flying is discouraged during the 15 days after treatment, because it could increase the chances of developing a venous thrombosis. If you have a flight planned, please tell us immediately so the treatment can be rescheduled.
- Immobilisation: in order to carry out sclerotherapy effectively and safely, we need the patient to be able to walk and move normally. A person with mobility difficulties or with total or partial immobilisation (for example, a plaster cast or splint) has an increased risk of potential complications (especially phlebitis and venous thrombosis), so this treatment is discouraged.
- Contraceptive treatments and similar therapies (menopausal hormone replacement, oncological treatments, etc): for many years we have known that this type of treatment causes more spider veins to appear, and faster, which makes treating them somewhat pointless (we will remove them on one side, but the hormonal treatment will soon cause new ones to appear). In addition, recent studies seem to suggest that people taking these types of hormonal treatments who undergo sclerotherapy may have a higher risk of serious adverse effects, such as phlebitis and venous thrombosis, which is why International Phlebology Guidelines are already beginning to advise withdrawing this type of treatment before performing sclerotherapy.
- Age: as usual, many risks and adverse effects increase with age. In the case of sclerotherapy, at least the risks of phlebitis and venous thrombosis clearly increase with age, so from around 65-70 years onwards your doctor should assess each case individually to decide whether the risk-benefit ratio is favourable or whether it is better not to perform this treatment.
The most important point is not to trivialise it: although we are seeking an aesthetic result, it is still a medical treatment. It must be indicated after a proper assessment and performed with appropriate safety measures.
FREQUENTLY ASKED QUESTIONS
Does sclerotherapy always remove spider veins?
A specific cosmetic result cannot be guaranteed. In most cases it clearly improves the treated reticular veins, but several sessions may be needed and the response varies between patients.
Do spider veins hurt or cause leg heaviness?
They do not cause pain, heaviness, or swelling by themselves. If there are symptoms in the leg, another cause should be looked for, especially true venous insufficiency.
Why is Duplex Ultrasound important before treatment?
Because it allows associated venous insufficiency and varicose veins to be ruled out or detected. If varicose veins are present, they must be assessed and treated before closing spider veins. It also makes it possible to detect potential situations that would make sclerotherapy ineffective, more likely to cause adverse effects, or even dangerous.
When are the results of sclerotherapy visible?
Results are not immediate. They usually start to be assessed from 4-6 weeks onwards, and the review is usually performed at 6-8 weeks.
Can post-sclerotherapy pigmentation be prevented?
The risk can be reduced by avoiding the sun, planning the timing of treatment carefully, and using the compression stocking correctly, but it cannot be prevented 100%.
Should you be interested in getting to know this disease better, and its causes, consequences, how to treat them, and, even better, what can we do to prevent them, you can find it all well explained in the ebook VARICOSE VEINS: Truth & myths.